
Introduction
Every year, the pharmaceutical industry in the United States develops several new pharmaceuticals that give significant medical benefits. Many of these drugs are expensive, contributing to increased healthcare expenses for both the private and federal governments. Policymakers have discussed strategies to slash prescription prices and minimise federal drug spending. Such rules would likely limit the industry’s incentive to create new medications.
Every year, the pharmaceutical industry in the United States creates a new class of medications that give significant medical benefits. Many of these drugs are expensive, contributing to increased health-care expenses in both the private and public sectors. Policymakers have examined strategies to reduce drug prices and federal drug spending. Such rules would likely limit the industry’s incentive to create new medications.
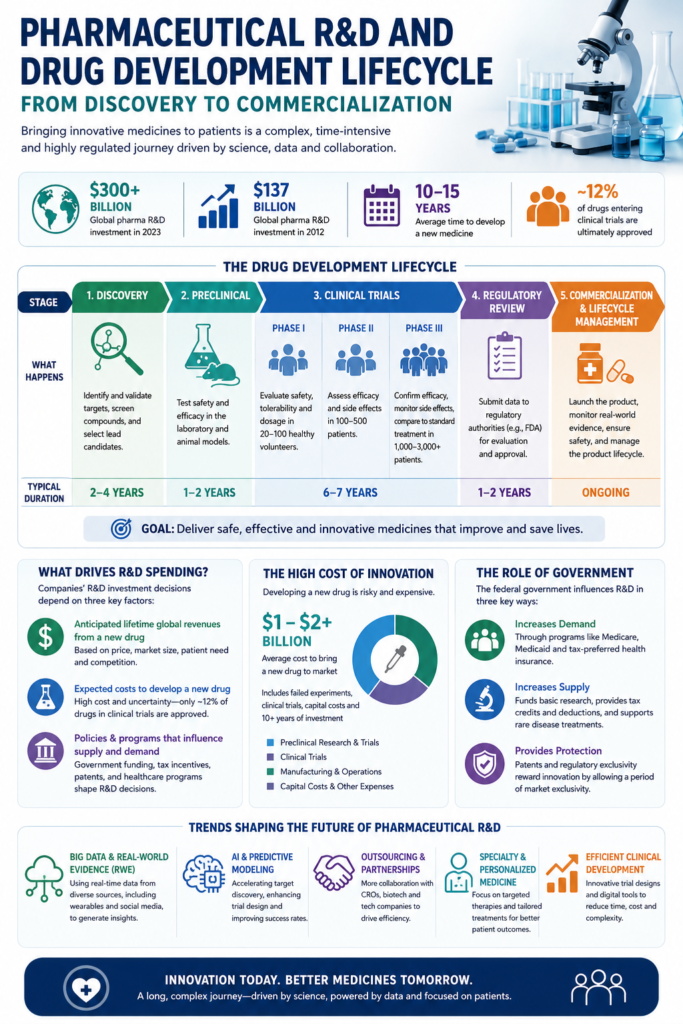
In 2023, pharmaceutical sector R&D investment will top $300 billion USD globally. In comparison, R&D spending reached 137 billion dollars in 2012. Pharmaceutical R&D encompasses all stages of disease process research, compound testing, pre-clinical development, and clinical trials. At some point in the process, usually during the pre-clinical phase, a governmental entity gets involved to review, regulate, and finally approve the product. In the United States, the Food and Drug Administration is the primary body responsible for procedures.
The pressure to innovate
In comparison to other industries, pharmaceutical companies are more driven by the imperative to manufacture innovative products, and thus to spend significant amounts on research and development. This is largely due to the time-limited patent protection of drugs and the following threat of sales erosion through generic and biosimilar competition. Two major effects of patent expirations for the pharma industry are a specific high R&D intensity and a growing focus on specialty drugs to diversify their product portfolio.
For the last several years, major developments in pharmaceutical research and development have begun to change the R&D landscape. A growing number of drug manufacturers are outsourcing large parts of R&D, mostly to clinical research organizations (also contract research organizations), with the main aim to reduce costs. Another important development is the use of big data in clinical research. Thus, a predictive modeling is possible which uses clinical and molecular data to develop safer and more efficient drugs. Particularly, real-time or real-world evidence (RWE) is becoming a greater interest. This makes cooperation with technology companies necessary and includes data gathered from various sources, even that of social media.
What Factors Influence Spending for R&D?
Drug companies’ R&D spending decisions depend on three main factors:
- Anticipated lifetime global revenues from a new drug,
- Expected costs to develop a new drug, and
- Policies and programs that influence the supply of and demand for prescription drugs.
Various considerations inform companies’ expectations about a drug’s revenue stream, including the anticipated prices it could command in different markets around the world and the expected global sales volume at those prices (given the number of people who might use the drug). The prices and sales volumes of existing drugs provide information about consumers’ and insurance plans’ willingness to pay for drug treatments. Importantly, when drug companies set the prices of a new drug, they do so to maximize future revenues net of manufacturing and distribution costs. A drug’s sunk R&D costs—that is, the costs already incurred in developing that drug—do not influence its price.
Developing new drugs is a costly and uncertain process, and many potential drugs never make it to market. Only about 12 percent of drugs entering clinical trials are ultimately approved for introduction by the FDA. In recent studies, estimates of the average R&D cost per new drug range from less than $1 billion to more than $2 billion per drug. Those estimates include the costs of both laboratory research and clinical trials of successful new drugs as well as expenditures on drugs that do not make it past the laboratory-development stage, that enter clinical trials but fail in those trials or are withdrawn by the drugmaker for business reasons, or that are not approved by the FDA. Those estimates also include the company’s capital costs—the value of other forgone investments—incurred during the R&D process. Such costs can make up a substantial share of the average total cost of developing a new drug. The development process often takes a decade or more, and during that time the company does not receive a financial return on its investment in developing that drug.
The federal government affects R&D decisions in three ways. First, it increases demand for prescription drugs, which encourages new drug development, by fully or partially subsidizing the purchase of prescription drugs through a variety of federal programs (including Medicare and Medicaid) and by providing tax preferences for employment-based health insurance.
Second, the federal government increases the supply of new drugs. It funds basic biomedical research that provides a scientific foundation for the development of new drugs by private industry. Additionally, tax credits—both those available to all types of companies and those available to drug companies for developing treatments of uncommon diseases—provide incentives to invest in R&D. Similarly, deductions for R&D investment can be used to reduce tax liabilities immediately rather than over the life of that investment. Finally, the patent system and certain statutory provisions that delay FDA approval of generic drugs provide pharmaceutical companies with a period of market exclusivity, when competition is legally restricted. During that time, they can maintain higher prices on a patented product than they otherwise could, which makes new drugs more profitable and thereby increases drug companies’ incentives to invest in R&D.
Third, some federal policies affect the number of new drugs by influencing both demand and supply. For example, federal recommendations for specific vaccines increase the demand for those vaccines and provide an incentive for drug companies to develop new ones. Additionally, federal regulatory policies that influence returns on drug R&D can bring about increases or decreases in both the supply of and demand for new drugs.
Every new drug product will follow its unique path toward the commercialization process. However, most novel drugs will go through three stages:
- Development (early)
- Commercialization (middle)
- Generic competition (late)
Let’s break down each of these three life cycle periods and the strategies for success.
New drug development
Also known as drug discovery, this initial process seeks new medicines to treat and cure ailments and diseases. The underlying goal is to identify new compounds that could have the desired palliative effect on the human body and establish the compound’s quality, safety, and efficacy for treating patients.
According to researchers, precious few new drugs survive this daunting process: “Of 5,000 compounds that enter pre-clinical testing, only five, on average, are tested in human trials, and only one of these five receives approval for therapeutic use.”
As mentioned, this incremental process typically takes more than a decade to finish and will cost more than a billion dollars. That’s because you must successfully pass through the various stages and series of actions, which include:
Stage 1: Early drug discovery
Researchers seek to identify genes connected to diseases or ailments, identify and authenticate proteins that cause the disease, and identify new compounds to prevent or assuage the disease. This consists of several pre-clinical steps, including:
- Target identification and validation
- High throughput screening
- Hit identification and discovery
- Assay development and screening
- Hit-to-Lead
- Lead optimization and generation

Stage 2: Pre-clinical phase
Once the target substances have been identified, researchers can start pre-clinical testing. Typically, these are performed on animals to identify lead candidates, develop the best drug scale-up procedures, find the optimal formulation and, satisfy regulatory safety and efficacy data requirements before they are permitted to move into clinical trials in humans.
Stage 3: Clinical phases
After animal tests have concluded, the pharmaceutical company will file an Investigational New Drug Application (INDA2). If approved, a new drug must pass through three phases of clinical trials:
Phase 1: A small group of healthy subjects (20 to 80) tests the tolerance and safety of the drug candidate. It answers questions like: is it safe, what is the ideal dosage, and how does the substance interact with the body?
Phase 2: In the next stage, larger groups (100 to 500 adult patients) begin to test the effectiveness, tolerability, and dosage.
Phase 3: In the final phase, doctors test the drug on groups of thousands of patients to determine whether it is safe and effective.
Stage 4: Regulatory approval – Having all the essential documents for clinical trials is important. Otherwise, it’s difficult to reach this stage. The few drugs that emerge from the unscathed clinical trials will submit their data and research to governing authorities for analysis. The company files a New Drug Application (NDA) covering all pre-clinical and clinical trial data. If the FDA approves the application, the company will begin post-market monitoring to further confirm the safety and efficacy of the new drug—especially compared to alternative treatments.
At each milestone, the stakes increase and so does the importance of tools that improve collaboration and insights generation. Those tools must break down data silos, aggregate and present unstructured data and ultimately prove their worth by accelerating time to milestone achievement.
Clinical trial design, including enrollment, retention and operations is the stage in pharma lifecycle management that the Within3 platform reaches robust milestone acceleration and ROI potential, especially among medical affairs teams for KOL engagement..
The COVID-19 pandemic has not only re-emphasized the importance of well-designed randomized clinical trials but also highlighted the need for large-scale clinical trials structured according to a master protocol in a coordinated and collaborative manner. – The Lancet
Check out our Guide to Effective Clinical Trial Design.
Strategies for pharmaceutical development
Since approximately just one in 5,000 compounds will ever make its way to market; small pharmaceutical companies must go above and beyond to position themselves for success. Today, patient-centricity lies at the heart of such efforts. To that end, HHS and the FDA recommended that companies deploy the following strategies for a patient-first focus:
Collect comprehensive and representative input – Pharma company teams must gather accurate patient insights from all relevant stakeholders to ensure that individuals are heard and considered for quality assurance.
Discover what matters to patients – Here, the patient experience matters deeply. Pharmaceutical companies must understand what matters to patients to design the most effective, accommodating, and applicable clinical trials possible.
Identify the insights that matter – With so much feedback, it can be challenging to sift through all of the data to find the insights that can be applied to create a successful market strategy.
Gather, store, and analyze clinical outcome assessment (COA) data – COAs should be woven into decision-making to ensure a patient-centric approach to drug development and pharma life cycle management.
An insights management platform closes the insight gaps detrimental to the new drug development regulatory process. This technology can identify, engage, and analyze input from medical affairs, clinical, commercial, internal, and payer groups worldwide to help you answer your most pressing questions.
With technologies like natural language processing and sentiment analysis, you can fine-tune your trial processes, identify new target markets, strengthen relationships with key opinion leaders (KOLs), and prevent costly mistakes or delays that so often occur because of the insights gap.
But where does this leave the big data element of AI for medical affairs within pharma lifecycle management?
“Given all that AI can do for pharma, the current state of AI for medical affairs is a promising opportunity to augment human expertise by extracting and capturing the most relevant data from stakeholders, ensuring its integrity, and then deciding what action to take based on insights generated from that data or information.”
By parsing EMR data, AI improves trial recruitment by identifying populations with the best chance of responding to treatment. AI is being used to replace placebo control groups with ‘digital twins’ of subjects for randomized clinical trials, allowing clinical teams to reduce the size of their control groups and minimize patient disruption.
AI applications are also being used to clean, aggregate, store, and manage clinical big data – helping clinical teams inform better site selection, optimize study designs, and accelerate the informed consent process. Predictive AI models can be used to calculate the results of a given treatment on a subject or group of subjects – potentially removing the need for animal testing and accelerating the preclinical phase. And finally, AI-powered wearable technologies are invaluable to clinicians as patient monitoring tools, enabling automatic detection of physical states.
Read more about the state of AI for medical affairs from our June 2024 blog: the bullet from the industry leaders, start small. Start with a pilot. Validate the desired efficiency gain or affect, then start to deploy AI more broadly.
What about AI’s implication and application for patient engagement?
From our February 2024 blog, the closest point of care for clinicians, AI currently supports the provision of care by:
Reducing administrative burden and improving patient engagement
Summarizing long documents and highlighting certain aspects of them, clinical trial reports, case studies, or care guidelines
Authoring a document with instructions from the physician or clinician, like a letter justifying a procedure to a payer
Provision of notes about patients’ conditions in their own language, in age-appropriate terms of understanding in some cases
“Saving four minutes on notes when minutes matter over the course of time and multiples of patients at a time when demands on clinicians related to numbers of patients seen is very high has a great deal of value.” – International Society for Pediatric Innovation
Pharmaceutical companies and their leaders know they will need AI to remain competitive in their respective races to identify promising new candidates, achieve regulatory approval, market adoption, patient access, and improve outcomes. Still, questions remain about how to safely onboard generative AI technology and how to use it ethically when communicating with and engaging patients.
Commercialization
Also known as the market exclusivity period, this stage covers the years between the launch of a new drug and the market launch of its first generic.
The market exclusivity period can be broken down into four sections:
Introduction to market – Early drug launch is primarily concerned with building stakeholder education and awareness, establishing patient support programs, forming partnerships with KOLs, and marketing the product.
Growth – As the company begins to grow and make a profit, leaders will seek to maximize market share and turnover.
Maturity – After a certain point, the growth of a pharmaceutical product is capped. Once maximum growth has been achieved, the focus shifts toward maintaining market share.
Decline – Eventually, profits and market share decline. In response, the company seeks to consolidate market segments and reduce expenses.
Strategies for commercialization
The commercialization process isn’t easy. Even if a new product makes it this far, success’s not guaranteed. That said, if you deploy the following strategies, you can increase the odds that your product can establish a foothold:
Practice supply chain management – One of the most important juggling acts involves physically bringing the product to the market without detracting from product quality. Product lifecycle management involves four major facets, including packaging & labeling, inventory management & transportation, product distribution, and product tracking and tracing. Here, practicing demand management and utilizing available technologies can facilitate all aspects of supply chain management.
Level up launch excellence – As we’ve previously written, successful drug launch is an event that results from the work of high-performing teams. Yet from 2009 to 2017, 40% of drug launches failed to meet their two-year sales goals. As a result, many pharma companies are forming pharma launch excellence teams to anticipate and avoid potential difficulties. Explore more in our blog on launch excellence.
Monitor post-launch success – Post-launch success requires constant campaign tweaking and optimization. But, to make the best decisions possible, you’ll need to carefully monitor the relevant KPIs.
Know and speak to your customer – There are three major reasons why a product development fails to launch: lack of communication, insufficient value propositions, and poor competitor understanding. If you want to capture the largest audience possible, you must purposefully address these common issues.
An insights management platform could provide significant value to your pharma marketing and commercialization efforts, especially when it comes to monitoring your post-launch data, better understanding customers, and improving communication between stakeholders at every stage in a new pharmaceutical product’s life cycle.
Effectively identifying and addressing slower than anticipated adoption: a mini case study
A medical leader was charged with discovering why a therapy had slower than anticipated adoption after two years on the market despite better clinical efficacy compared to the standard of care. Information was difficult to access and integrate, siloed through different parts of the organization from the field, information from congresses, online, social listening, advisory boards, medical information and so on.
To mine the high volume and multiple types of information to understand what’s really happening in the marketplace the team implemented a third generation AI tool to collectively analyze data from multiple sources, including field data, clinical trial data, advisory boards, and social listening.
They found that 22% of the relevant HCPs had no knowledge at all of the treatment. They learned that they didn’t really have KOLs, they had STLs – the same 12 leaders. They met with the same 12 leaders all the time for everything. The familiarity of the company with those KOLs and vice-versa was distorting their view of how expansive, or limited, their education efforts have been.
Because their delivery mechanism and market access was complex as well, they hadn’t really understood the relationship that access difficulty is directly related to interest in and learning about a therapy. They weren’t appreciating the interrelationship between the difficulty of access and lack of education.
The process-improved learnings drove hundreds of hours of savings and extended the market share opportunity by more than 40%.
Generic competition
The final stage is when the exclusive patent for the pharmaceutical product expires. This is what’s known as the “drug patent cliff.”
At this point, generic competition can enter the market and eat away at a company’s market share and profits. As a result, the drug’s average price drops dramatically, as does the branded drug’s market share.
During the late stage of the pharmaceutical lifecycle, the goal is to minimize market share loss. Strategies you can deploy to accomplish this include:
Evergreening – By either extending the line of releasing a next-generation version of the drug product, a company seeks to transition existing and would-be clients from the older drug to the newly patented product. Ideally, this is done to prevent loss of exclusivity.
Pediatric licensing – If the drug was exclusively used for adults, another loss of exclusivity countermeasure would be to expand its usage to children. Doing so could temporarily delay patent expiry.
Maximizing profits – Many pharmaceutical companies seek to maintain or raise prices before the patent cliff. Then, after the patent has expired, they can mitigate losses by offering patient rebates, vouchers, or adherence programs.