
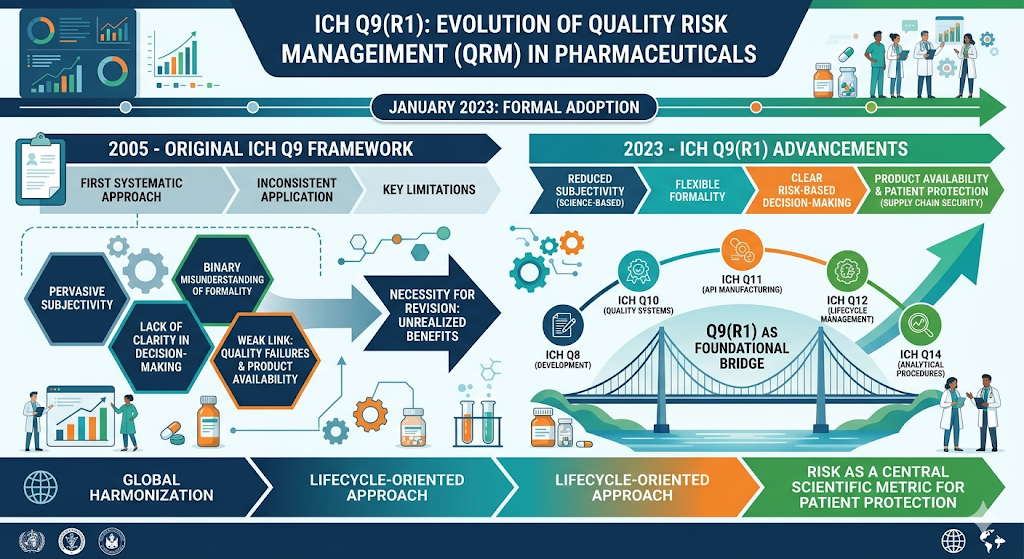
The formal adoption of the ICH Q9(R1) guideline in January 2023 represents a pivotal advancement in the global harmonization of pharmaceutical quality standards, addressing nearly two decades of implementation experience and evolving industrial complexities. Originally introduced in 2005, the ICH Q9 framework provided the first systematic approach to Quality Risk Management (QRM) within the pharmaceutical sector, yet its application remained inconsistent across global regulatory jurisdictions and manufacturing operations. The R1 revision was necessitated by the recognition that the full benefits of QRM—as envisioned in the mid-2000s—had not been realized due to pervasive subjectivity, a binary misunderstanding of formality, a lack of clarity in risk-based decision-making, and an insufficient link between quality failures and product availability. By refining these pillars, ICH Q9(R1) serves as a foundational bridge to other quality guidelines, including ICH Q8, Q10, Q11, Q12, and Q14, fostering a lifecycle-oriented approach where risk is not merely an administrative hurdle but a central scientific metric for patient protection.
The Historical Trajectory and Implementation Necessity of the R1 Revision
The path to ICH Q9(R1) began with the approval of a Concept Paper in November 2020 and a subsequent Business Plan, reflecting a consensus among the ICH Expert Working Group (EWG) that the original guidance required targeted adjustments rather than a complete overhaul. The revision process followed the standard ICH Step process, navigating through draft endorsement (Step 2) in November 2021 to a substantial public consultation phase (Step 3) that garnered approximately 775 comments from stakeholders globally. This feedback mechanism was critical in ensuring that the final Step 4 document, finalized on 18 January 2023, addressed the practical realities of pharmaceutical manufacturing and regulatory oversight.
| Guideline Development Phase | Date | Key Outcome and Regulatory Impact |
| Initial Step 4 Adoption | 9 November 2005 | Established the global standard for QRM implementation. |
| Concept Paper Approval | 13 November 2020 | Identified the four core areas for improvement: Subjectivity, Product Availability, Formality, and Decision-Making. |
| Step 2 Endorsement | 18 November 2021 | Released the draft revision for global public review. |
| Step 3 Consultation Completion | March 2022 | Evaluated 775 comments to achieve cross-regional consensus. |
| Final Step 4 Adoption | 18 January 2023 | Finalized the R1 guideline for implementation by regulatory members. |
| FDA Implementation (Step 5) | May 2023 | The United States published the final guidance for domestic industry. |
The impetus for this revision was also deeply influenced by the global supply chain vulnerabilities exposed during the 2020-2022 period. The regulatory community recognized that manufacturing quality problems and non-compliance with Good Manufacturing Practice (GMP) were not only compliance issues but were primary drivers of drug shortages that directly impacted patient care. The shift in terminology from ‘Risk Identification’ to ‘Hazard Identification’ further exemplifies the drive toward scientific rigor, ensuring that the identification of potential sources of harm is distinct from the subsequent analysis of risk probability and severity.
Theoretical Foundation: The Formality Continuum in Quality Risk Management
One of the most significant structural changes in ICH Q9(R1) is the elaboration on “formality” within Section 5.1. For much of the 2005-2022 era, industry practitioners viewed formality as a binary state: an exercise was either “formal”—requiring extensive documentation and complex tools like Failure Mode and Effects Analysis (FMEA)—or “informal,” which often implied a lack of documentation or scientific depth. The R1 revision clarifies that formality is a continuum, ranging from low to high, and that the degree of rigor applied should be commensurate with the level of risk, uncertainty, importance, and complexity of the issue at hand.
Determinants of Formality and Resource Allocation
The revised guideline posits that an organization’s Quality Management System (QMS) should define the criteria for determining the appropriate level of formality. This determination is not arbitrary but is driven by a synthesis of three primary factors: Importance, Complexity, and Uncertainty. The relationship can be expressed through a conceptual framework where the depth of the QRM process is a function of these variables:
Degree of Formality=f(Importance,Complexity,Uncertainty)
In this context, Importance refers to the potential impact on product quality and patient safety; Complexity involves the number of variables, interfaces, or multidisciplinary inputs required; and Uncertainty reflects the lack of knowledge or predictability regarding the process or hazard. High uncertainty combined with high complexity necessitates a high-formality approach, including the use of stand-alone QRM reports and trained facilitators. Conversely, simple, well-understood changes can be managed with lower formality, often embedded within existing QMS elements like change control or deviation management records.
| Formality Driver | Characteristic of High Formality | Characteristic of Low Formality |
| Methodology | Use of structured tools like FMEA, HACCP, or FTA. | Use of checklists, brainstorming, or narrative rationales. |
| Team Structure | Large, multidisciplinary team with independent facilitators. | Individual SME or a small, focused group. |
| Documentation | Extensive, stand-alone risk reports with detailed appendices. | Risk-based rationale recorded within standard QMS forms. |
| Causal Analysis | Deep Root Cause Analysis (RCA) including secondary factors. | Identification of primary immediate causes. |
| Knowledge Use | Explicit elicitation of expert opinion and probabilistic modeling. | Reliance on existing process experience and standard data. |
The industry has noted that the previous lack of clarity led to the “over-engineering” of simple risk assessments, which consumed excessive resources without adding scientific value, or the “under-engineering” of complex risks, which resulted in significant quality defects. By providing a spectrum, ICH Q9(R1) allows organizations to optimize resource allocation, focusing the highest level of scientific rigor on the most critical threats to patient safety.
Behavioral Science and the Mitigation of Subjectivity
Subjectivity has been identified as a persistent barrier to effective QRM, often leading to inconsistent risk assessments and divergent regulatory outcomes. Section 5.3 of the revised guideline introduces the concept of “Managing and Minimizing Subjectivity,” acknowledging that while absolute objectivity may be unattainable, the influence of personal opinions, cognitive biases, and heuristics must be controlled.
Subjectivity typically enters the QRM process through:
- Perceptual Differences: Stakeholders may perceive hazards, harms, and risks differently based on their specific professional background or organizational role.
- Poorly Designed Tools: The use of risk scoring scales with ambiguous definitions (e.g., vague labels for “high” or “low”) can lead to inconsistent scoring among different teams.
- Heuristics and Biases: Cognitive behaviors such as “groupthink,” availability bias, and anchoring can skew the estimation of probability and severity.
Strategies for Objective Risk Evaluation
To mitigate these factors, ICH Q9(R1) emphasizes the use of science-based control strategies and the maximization of relevant data sources. This is where the cross-reference to ICH Q10 Section 1.6.1 becomes critical; Knowledge Management (KM) is positioned as the primary tool for reducing subjectivity. By grounding risk assessments in historical process data, validation studies, and deviation records, teams can move away from qualitative guesswork toward quantitative or semi-quantitative analysis.
Structured techniques recommended for reducing subjectivity include the use of trained facilitators who can identify and neutralize biases during team discussions, and the implementation of formal expert elicitation protocols like the Cooke’s classical model. These protocols involve calibrating experts using “seed questions” for which the true values are known, thereby weighting the opinions of those with demonstrated statistical accuracy more heavily in the final risk output. Such rigorous approaches are particularly justified in high-formality scenarios where the uncertainty is significant and the importance to patient safety is high.
Risk-Based Decision-Making: Uncertainty and Knowledge Management
Risk-Based Decision-Making (RBDM) is highlighted in Section 5.2 as an essential foundation for organizational governance. Effective RBDM involves a structured process of weighing options under conditions of uncertainty, using knowledge to facilitate informed choices. The revised guideline suggests that there are varying degrees of structure for RBDM, which correspond to the formality continuum.
The decision-making process in QRM generally includes:
- Identifying the specific hazards and associated risks.
- Determining the necessary risk controls to mitigate those risks to an acceptable level.
- Evaluating the acceptability of the residual risk.
- Managing the communication and review of the decision throughout the product lifecycle.
A key insight from the R1 revision is the distinction between “rule-based” and “risk-based” decisions. Rule-based decisions are often binary and based on fixed specifications, whereas risk-based decisions address uncertainty by evaluating multiple causal factors and the potential for unintended consequences of a change. The guideline explicitly links this to Knowledge Management, stating that as all decision-making relies on knowledge, the principles of ICH Q10 must be integrated to ensure that the best available information is used to resolve uncertainty.
Quality Risk Management in the Context of Product Availability
One of the most profound additions in the R1 revision is Section 6.1, which addresses the role of QRM in mitigating product availability risks. The definition of “harm” in the context of pharmaceutical quality has been expanded to explicitly include damage resulting from a “loss of product availability”. This recognizes that a medicine that is not available to a patient—due to a manufacturing failure or GMP non-compliance—poses a risk as significant as a quality defect in the product itself.
Data from 2018 to 2024 reveals a stark reality: manufacturing and quality issues cause over 60% of drug shortages. The fragility of the global supply chain, where 80% of Active Pharmaceutical Ingredients (APIs) are manufactured in regions like China and India, increases the systemic risk of shortages. In April 2025, for example, Glenmark Pharmaceuticals recalled 40 generic medications due to cGMP violations involving cross-contamination and testing method validation failures, highlighting how quality lapses lead directly to supply disruption.
| Shortage Metric | Data Point | Context and Implication |
| Duration of Shortages | 4.6 years (Injectables) vs. 1.6 years (Oral) | Injectables face higher manufacturing complexity and lower profitability. |
| Primary Cause of Shortage | >60% due to manufacturing/quality problems | Highlights the critical link between QRM and supply continuity. |
| API Dependency | 80% manufactured in China and India | Creates “systemic fragility” vulnerable to natural disasters or trade issues. |
| New Shortages in 2024 | 15 (Decreased from peak of 251 in 2011) | Early notification requirements are helping, but active shortages remain high. |
| Critical Drug Impact | 1/3 are Essential Medicines | Shortages of oncology and ICU agents pose life-or-death threats to patients. |
The R1 revision emphasizes that an effective PQS should use QRM and KM as an “early warning system” to detect and respond to evolving quality risks before they manifest as supply disruptions. This proactive approach involves monitoring manufacturing process variation, facilities and equipment health, and the oversight of outsourced activities. Specifically, Section 6.1 and Annex II.9 drive the industry to treat supply chain robustness and sustainable GMP compliance as inseparable objectives.
Semantic Rigor: From Risk Identification to Hazard Identification
The shift from ‘Risk Identification’ to ‘Hazard Identification’ in the R1 guideline is more than a simple terminology change; it represents a commitment to semantic precision in the risk assessment process. This alignment with the established definition of risk assessment ensures that teams first focus on identifying the hazard—a potential source of harm—before analyzing the risk, which is the combination of probability and severity.
Risk=P(Occurrence of Harm)×S(Severity of Harm)
When teams are tasked with “Risk Identification,” they often begin estimating probability and severity too early, leading to cognitive fatigue and the overlooking of actual hazards. By isolating Hazard Identification as the first step, the process becomes more robust, ensuring that all potential failure modes are captured without the distraction of early evaluation. While past risk assessments do not need to be retrospectively updated, future QRM work must adopt this terminology to maintain global harmonization.
Integration with the Pharmaceutical Quality System (ICH Q10)
ICH Q9(R1) serves as a critical enabler for the ICH Q10 Pharmaceutical Quality System. There are four primary cross-references to Q10 within the R1 text, specifically highlighting Knowledge Management (Section 1.6.1) and the Management of Outsourced Activities and Purchased Materials (Section 2.7).
The synergy between these guidelines creates a lifecycle approach:
- Pharmaceutical Development (ICH Q8): QRM is used to build knowledge and understand risk scenarios during process design.
- Commercial Manufacturing: QRM informs the control strategy, guiding the monitoring of Critical Process Parameters (CPPs) and Critical Quality Attributes (CQAs).
- Post-Approval Changes (ICH Q12): QRM enables an “optimized science and risk-based” change management process, where high-formality assessments ensure that changes do not negatively impact the validated state.
- Discontinuation: QRM is used to manage the final stages of the product lifecycle, ensuring that patient needs are met until the product is safely transitioned.
Furthermore, the revision underscores the responsibility of senior management to lead the PQS. The effectiveness of a PQS is demonstrated through its ability to apply QRM principles proactively, fostering a quality culture that rewards candor and recognizes the strategic importance of risk-based thinking.
Implementation Science and Training Materials
To support the transition to R1, the ICH EWG developed a suite of new training materials, including 36 PowerPoint presentations and case studies. These materials are essential because the previous training suite (2006-2010) contained discrepancies that conflict with the revised guidance—specifically regarding the binary view of formality and the term ‘Risk Identification’.
Implementation considerations for organizations include:
- Revising SOPs: Updating quality procedures to reflect the formality continuum and the three drivers (Uncertainty, Importance, Complexity).
- Team Training: Ensuring that risk assessment teams understand the impact of cognitive biases and the importance of scientific knowledge over subjective opinion.
- Supplier Oversight: Integrating product availability risks into supplier quality agreements and audit protocols as per Section 2.7 of ICH Q10.
- Digitalization: Recognizing that emerging technologies like advanced data analysis can reduce risk but may also introduce new challenges that require their own QRM application.
Synthesis of Industry Impact and Future Outlook
The release of ICH Q9(R1) marks a transition from “administrative QRM” to “scientific QRM”. By addressing the four critical areas of deficiency, the guideline empowers both industry and regulators to conserve resources while enhancing the safety and availability of medicines. The evolution toward high-maturity quality systems, as seen in programs like the FDA’s Quality Management Maturity (QMM) initiative, relies heavily on the robust application of the R1 principles.
In conclusion, the R1 revision of ICH Q9 is a foundational pillar for a modern, resilient pharmaceutical supply chain. It redefines quality as a multidimensional construct that encompasses not just the physical integrity of the product, but the systemic reliability of the processes that deliver it to the patient. As organizations integrate these principles, the industry can expect more effective, data-driven decisions, fewer quality-related supply disruptions, and a significant improvement in the global protection of public health. The move toward minimizing subjectivity through Knowledge Management, combined with a flexible but rigorous formality spectrum, ensures that Quality Risk Management remains a value-adding discipline throughout the twenty-first-century pharmaceutical lifecycle.

ICH Q9 revision Quality Risk Management.pdfdatabase.ich.orgFinal Concept Paper ICH Q9(R1) – Quality Risk Management 24 March 2023 Endorsed by the Management Committee on 4 April 2023 TypeOpens in a new windowdatabase.ich.orgquality risk management q9(r1) – ICHOpens in a new windowoutsourcedpharma.comRisk Tool Selection With ICH Q9(R1) In Mind – Outsourced PharmaOpens in a new windowdatabase.ich.orgQuality Risk Management, ICH Q9(R1)Opens in a new windowfda.govOverview of Changes: ICH Q9 (R1) Quality Risk Management – FDAOpens in a new windowfda.govQuality Risk Management, ICH Q9(R1) – FDAOpens in a new windowipq.orgICH Q9(R1) and some personal thoughts about implementing the new guidance | IPQ.orgOpens in a new windowfda.govQ9(R1) Quality Risk Management – FDAOpens in a new windowdatabase.ich.orgICH Q9(R1) EWG Work Plan August 01, 2022Opens in a new windowintuitionlabs.aiICH Q10 Guide: Implementing a Pharmaceutical Quality System – IntuitionLabsOpens in a new windowdatabase.ich.orgquality risk management q9(r1) – ICHOpens in a new windowdatabase.ich.orgICH Q9(R1) EWG Work Plan January 24, 2022Opens in a new windowfda.govQ9(R1) Quality Risk Management – FDAOpens in a new windowfda.govQ9(R1) Quality Risk Management May 2023 – FDAOpens in a new windowncbi.nlm.nih.govAnalysis of Drug Shortages, 2018-2023 – NCBI BookshelfOpens in a new windowfda.govDrug Shortages Report to Congress | Calendar Year 2024 – FDAOpens in a new windowpharmacytimes.comLong-Lasting Drug Shortages Highlight Fragile Supply Chains and Systemic Market Pressures | Pharmacy TimesOpens in a new windowinvestigationsquality.comWhy the Shift to Hazard Identification in ICH Q9(r1) Matters – Investigations of a DogOpens in a new windowregdevinc.comICH-Q9(R1): Formal Revision to Quality Guideline for Quality Risk ManagementOpens in a new windowjddtonline.infoQuality Risk Management: Degree of formality, Formal and Informal QRMOpens in a new windowema.europa.euOverview of comments received on ICH guideline Q9 (R1) on quality risk management (EMA/CHMP/ICH/24235/2006)Opens in a new windowoutsourcedpharma.comICH Guideline Q9(R1) On QRM Part 1 Formality Risk-based Decisions – Outsourced PharmaOpens in a new windowpharmtech.comNavigating the Formality Spectrum in ICH Q9(R1) – Pharmaceutical TechnologyOpens in a new windowscribd.comICH Q9 (R1) Formality Training Material 2023 0929 | PDF | Risk – ScribdOpens in a new windowinvestigationsquality.comTag: formality in QRM – Investigations of a DogOpens in a new windowcollections.nlm.nih.govQ9(R1): : quality risk management : guidance for industry – NLM Digital CollectionsOpens in a new windowinvestigationsquality.comReducing Subjectivity in Quality Risk Management: Aligning with ICH Q9(R1)Opens in a new windowfda.govReport on the State of Pharmaceutical Quality FY2024 – FDAOpens in a new windowdatabase.ich.orgICH Q10 Pharmaceutical Quality System (PQS)Opens in a new windowpharmtech.comShining a Light on the Long Shadow of Subjectivity in Quality Risk ManagementOpens in a new windowdatabase.ich.orgICH Q9(R1) EWG Work Plan February 24, 2023Opens in a new windowqualio.comICH Q10 compliance checklist – QualioOpens in a new windowfda.govKnowledge Management: An Iterative Process | FDAOpens in a new windowdatabase.ich.orgquality risk management q9(r1) – ICHOpens in a new windowbpi.bioprocessintl.comICH Q9(R1) Quality Risk Management Revision – Public ConsultationOpens in a new windowslideshare.netICH Q9R1_Step_4_Presentation_2023_0314_final.pdf – SlideshareOpens in a new windowfda.govDrug Shortages – FDAOpens in a new windowpmc.ncbi.nlm.nih.govKey Drivers and Mitigation Strategies of Oncology Drug Shortages 2023 to 2025 – PMCOpens in a new windowpharmaceuticalcommerce.comQuality and Compliance in the Pharmaceutical Industry: Navigating a Transformed LandscapeOpens in a new windowpharmexec.comTop Drugs at Risk of Supply Shortages: Report | PharmExecOpens in a new windowarrow.tudublin.ieICH Q9(R1): The Quality Leader’s Opportunity for Effective, Patient-centric Decision-makingOpens in a new windowpmc.ncbi.nlm.nih.govICH Q10 PHARMACEUTICAL QUALITY SYSTEM GUIDANCE: UNDERSTANDING ITS IMPACT ON PHARMACEUTICAL QUALITY – PMCOpens in a new windowipqpubs.comINTERNATIONAL PHARMACEUTICAL QUALITY™ – IPQpubsOpens in a new windowdatabase.ich.orgICH Q9(R1): Quality Risk ManagementOpens in a new windowfederalregister.govQ9(R1) Quality Risk Management; International Council for Harmonisation; Draft Guidance for Industry; Availability – Federal RegisterOpens in a new windowarrow.tudublin.ieManaging Knowledge and Risk:a Literature Review on the Interdependenc