
The global pharmaceutical sector operates under a highly advanced and ever-evolving regulatory environment. With the emergence of new therapeutic modalities based on biologics, cell and gene therapies, and even artificial intelligence diagnostics, the role of national/regional regulators has transcended its historical role as the ultimate gatekeeper at the back end of product lifecycles. The assessment of safety, efficacy, and quality of such products calls for a great deal of expertise and robust quality systems that strike a balance between comprehensive scientific assessment and fast patient access.
The current regulatory environment can be described using two key terms – decentralization and departure from historical binary classifications. Although the United States FDA and EMA still remain the main regulatory reference points, the fast advancement of national regulators in Asia-Pacific and Latin America has changed the approach to global drugs development. At the same time, work-sharing arrangements, simultaneous review programs, and revised benchmarking approaches have created a networked system of regulation where sovereign regulators use joint scientific assessments for resource optimization and speedy market entry.
The Strategic Shift from Stringent Regulatory Authorities to WHO-Listed Authorities
For nearly two decades, international procurement agencies as well as national regulatory networks depended on the criteria of the Stringent Regulatory Authority (SRA) in making procurement decisions and establishing regulatory trust. Initiated by the WHO and the Global Fund back in 2008, the SRA criteria included historical participation in the ICH before October 2015, or legal arrangements of mutual recognition with ICH member countries. However, this concept faced criticism due to its geographical bias towards industrialized countries of the Global North and assumption of equal regulatory stringency for all product types without objective performance verification.
In an effort to provide a clear, unbiased, and evidence-based approach to the issue, the WHO developed the Global Benchmarking Tool (GBT) in 2016, forming the basis of the WHO-Listed Authority (WLA). The GBT assesses national regulatory authorities in nine fundamental regulatory functions, categorizing systems on a standard maturity scale from Level 1 to Level 4.
A maturity level 1 designation is assigned to systems that have inadequate or ad hoc regulatory capabilities while maturity level 2 designates evolving regulatory authority with oversight functions. For the WLA designation to take place, the national/regional regulatory authority should attain at least maturity level 3 (ML3) which describes a stable and integrated regulatory system. The maturity level 4 (ML4) on the other hand describes a high level of performance and continuous improvement.
After attaining ML3 or ML4, the candidate authorities undergo a Performance Evaluation (PE) to ensure that the consistent adherence to good regulatory practices and internationally recognized standards is attained. This new approach to WLA designation provides for the regulators to be designated as WLAs by specific functions or product categories.
To achieve this transition, WHO developed a five-year transitional arrangement that will end in March 2027 whereby the previously certified SRAs and the high performing authorities will be on a tWLA list before undergoing the formal evaluation process. An important milestone in this process was the designation of the EMRN as a WLA due to the advanced performance of the network including EC, EMA and the national competent authorities in the European Economic Area.
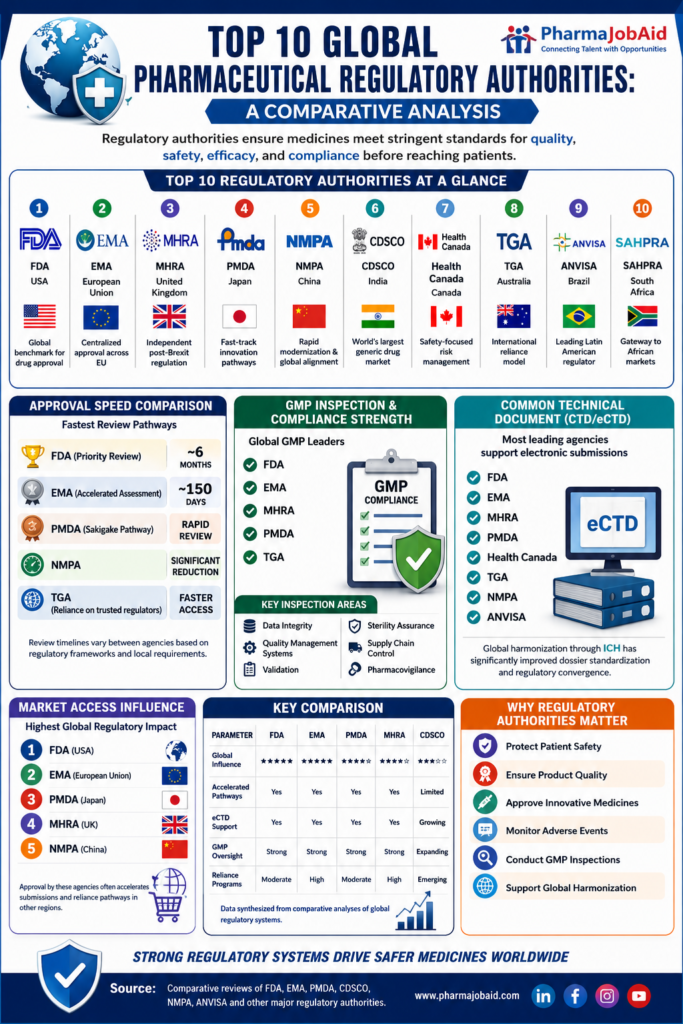
Comprehensive Profiles of the Top 10 Regulatory Authorities
[GLOBAL BIOPHARMACEUTICAL MARKET ENTRY]
|
________________________________|________________________________
| | |
v v v
[North America] [Europe & UK] [Asia-Pacific]
* US FDA (USA) * EMA (European Union) * PMDA (Japan)
* Health Canada * MHRA (United Kingdom)* CDSCO (India)
* Swissmedic (Swiss) * NMPA (China) [cite: 19]
* TGA (Australia)
|
v
[Latin America]
* ANVISA (Brazil)
1. Food and Drug Administration (FDA) – United States
With the mandate by the statutes of the Federal Food, Drug, and Cosmetic (FD&C) Act, the Food and Drug Administration of the United States FDA is among the most prominent regulatory authorities globally. The CDER and CBER Centers of the FDA regulate the approval of human drugs and biologics.
Sponsors have to go through specific clinical milestones beginning with the filing of an IND application to get the permission to conduct human trials. After collection of the clinical data, the marketing of the product is sought using NDA applications for chemical products or BLA application for biological products. Generic products are evaluated using ANDA application procedure that avoids lengthy clinical trials and only proves the bioequivalence with the reference listed drug.
The operational policies and procedures of the FDA are provided in the Title 21 of Code of Federal Regulations (21 CFR) with the 21 CFR Part 11 being the foundation of electronic record keeping and e-signature requirements. The high-risk products are managed using Risk Evaluation and Mitigation Strategies (REMS). In case the application does not meet the requirement, the agency issues a Complete Response Letter (CRL).
Medical devices are cleared and approved by the Center for Devices and Radiological Health of the FDA using the 510(k) pre-market notification process and Premarket Approval (PMA). From the financial point of view, FDA follows the user fee structure that is updated every year in the context of PDUFA, GDUFA, BsUFA, and MDUFA.
It is important to note that from 1 October 2025, the FDA stopped all paper payments for user fees and required all payments in USD.
2. European Medicines Agency (EMA) – European Union
The European Medicines Agency is the centralized agency that conducts scientific evaluation of the medications for human and veterinary use in the European Union, where it coordinates activities among more than thirty national competent authorities. Inventions having high scientific value, biotechnological medicinal products and orphan drugs should go through the Centralized Procedure, leading to one unique marketing authorization valid throughout all EU countries.
Packaging and labeling of the product should meet all criteria of the QRD template, and should be translated into all Union languages.
On January 1, 2025, the European Medicines Agency put into force the EU Regulation No 2024/568, which dramatically changed the financial model of this institution. The new regulation has substituted the outdated system of flat-rate assessments for a new proportionate fees approach making fees paid by marketing authorization holders proportional to the amount of work that should be done on each particular application.
In accordance with the mentioned regulation, the size of the fee for an application of MAA depends on the exact legal basis under which the application was submitted. The fee for the re-examination of the scientific opinion is calculated as 30% of the initial net fee for review.
To support and promote innovations of the smaller companies, the EMA provides a wide range of SME incentives, including postponement of the payment for re-examinations until the issuance of an administrative decision or withdrawal of the application.
3. Pharmaceuticals and Medical Devices Agency (PMDA) Japan
One of the features of the regulatory system of Japan lies in the allocation of the legal and technical aspects of regulation to the two co-dependent authorities – the Ministry of Health, Labour and Welfare (MHLW), which has the exclusive legal right to approve marketing authorizations and to determine public prices, and Pharmaceuticals and Medical Devices Agency (PMDA), which is an independent administrative agency conducting scientific “shinsa” (review) of drug, device and regenerative medicine applications.
One of the problems of the Japanese market used to be its serious “drug lag” or “drug loss” problem, in which the drugs developed abroad were delayed or were not launched in Japan owing to the need for conducting additional domestic clinical trials. The issue has been addressed through the amendment of MRCT requirements: starting from fiscal year 2023, domestic Phase I studies are no longer considered mandatory before joining global studies.
Also, according to the revised Pharmaceutical and Medical Device Act of 2025, sponsors filing an application for an adult drug should include the pediatric development plan in the package.
After receiving the marketing approval, a therapeutic product should be incorporated into the National Health Insurance (NHI) uniform public pricing scheme. Listings for new drugs are published quarterly in February, May, August, and November, and in February and April for generics. Uniform listing occurs within 60 days of the regulatory approval of the product, up to 90 days in the worst case scenario, thus, ensuring the market predictability.
PMDA uses the consultation-based review model, in which sponsors have to pay statutory fees for the formal meetings regarding safety, quality, and clinical trial exemption issues.
4. Medicines and Healthcare products Regulatory Agency (MHRA) – United Kingdom
After the United Kingdom’s withdrawal from the European Union, the Medicines and Healthcare products Regulatory Agency (MHRA) became an independent sovereign regulator. In its quest to maintain the attractiveness of the United Kingdom in regard to development of medicines, the MHRA has implemented flexible and visionary review systems.
The Innovative Licensing and Access Pathway (ILAP) is one of such initiatives aimed at making the approval of innovative treatments shorter through creation of a roadmap combining regulatory review, Health Technology Assessment (HTA) and authorization of clinical trials within one single structure.
In order to avoid problems related to the fact of having a smaller and single-nation market, the MHRA has made sure to join international initiatives that would promote work sharing, becoming one of the active participants of Access Consortium and Project Orbis.
5. Central Drugs Standard Control Organisation (CDSCO) – India
As the National Regulatory Authority of India working through the Ministry of Health and Family Welfare, CDSCO is tasked with the approval of new drug registration, clinical trials, and standardization of cosmetics & medical devices. The Drugs Controller General of India (DCGI) heads the organization and serves as the Central Licensing Authority.
The regulatory framework of India operates on central and state lines. While the central CDSCO regulates the importations, clinical trial and new drug registrations, the state-based State Drug Control Authorities have the prime role to license manufacturing sites locally, distribute products and carry out local inspections.
For any recombinant biologics, biosimilars and advanced therapies, the sponsor will need to work through an entire suite of agencies:
CDSCO: Acts as the prime agency, receiving all applications for marketing authorization and reviewing through its Subject Matter Expert Committees (SEC).
Review Committee on Genetic Manipulation (RCGM): This is an independent agency under the Department of Biotechnology (DBT) that will provide necessary approval for manufacturing of any recombinant products, import of gene therapy products and studies involving genetic manipulation.
Genetic Engineering Appraisal Committee (GEAC): This committee examines the large scale release of environment and biosafety issues related to genetically modified organisms.
National Institute of Biologicals (NIB)/Central Drugs Laboratory (CDL): Mandatory scientific lot release testing for all vaccines, blood products and sera.
Sponsors usually underestimate the multi-agency process and face delays in market launches due to this reason.
With regard to labeling, the Indian regulation mandates the bilingual requirement for packaging where all relevant information should be displayed in English and Hindi. On the operational side, the organization is moving from its SUGAM portal towards its Digital Drugs Regulatory System (DDRS).
6. National Medical Products Administration (NMPA) – China
Under the purview of the National Regulatory Authority of India via Ministry of Health and Family Welfare, CDSCO undertakes the responsibilities of new drug registration, clinical trials and standardization of cosmetics & medical devices. DCGI serves as the Head of CDSCO and acts as the Central Licensing Authority.
Regulatory structure of India is structured into central and state bodies. Whereas the central CDSCO will regulate importations, clinical trials and new drug registrations, the state-based State Drug Control Authorities will be the primary agencies licensing manufacturing facilities locally, distribution and inspections locally.
For all types of recombinant biological products, biosimilars and advanced therapies, sponsor needs to go through the process of multiple agencies
CDSCO: Will act as the prime agency receiving all applications of marketing authorization and their review via Subject Matter Expert Committees (SEC).
Review Committee on Genetic Manipulation (RCGM): This agency will give all approvals regarding the manufacture of recombinant products, importation of gene therapy products and genetic manipulations.
Genetic Engineering Appraisal Committee (GEAC): It will take up the examination of large scale release of environment and biosafety issues related to genetically modified organisms.
National Institute of Biologicals (NIB)/Central Drugs Laboratory (CDL): This agency will conduct mandatory scientific lot release testing of all vaccines, blood products and sera.
Sponsors usually underestimate this multi-agency process and face delays in their market launch because of this reason.
Whereas concerning labeling, there is a rule for bilingual requirement for packaging for all information in English and Hindi. Operational wise, the organization is shifting from its SUGAM portal to its DDRS.
7. Health Canada – Canada
The Health Products and Food Branch (HPFB) within Health Canada regulates human drugs, biologics and medical devices under the Food and Drugs Act and its Regulations. Approvals are issued in the form of Notices of Compliance (NOC) and Drug Identification Number (DIN) and all DIN holders have to obtain a Drug Establishment Licence (DEL) for their manufacturing, import and wholesale operations.
As far as biologics, which are evaluated by the Biologic and Radiopharmaceutical Drugs Directorate (BRDD) are concerned, Health Canada operates an innovative On-Site Evaluation (OSE) pre-market program. This is a product-specific evaluation performed on-site to confirm that CMC of a specific product can be carried out consistently to deliver a biologic that will be safe for use.
Compliance activities and enforcement are controlled by the Regulatory Operations and Enforcement Branch (ROEB) through the Health Product Compliance Directorate (HPCD). The Health Product Inspection and Licensing Division (HPIL) carries out domestic and international GMP inspections based on the cycle, risk-based approach when the average frequency of audit is four years. For foreign establishments of non-Mutual Recognition Agreement (MRA) countries HPIL gives a “New Evidence Required BY” (NERBY) date in order to assure ongoing GMP verification.
Health Canada also has a stringent system in place to mitigate drug shortages. According to new changes to the permanent Food and Drug Regulations (FDR) no DEL holder is allowed to export any Canadian labelled drug, which can result in shortage situation in Canada.
These changes were made specifically to prevent Canadian supply of medicines from being depleted by foreign bulk purchase schemes, including those in effect in US states since 2024.
8. Therapeutic Goods Administration (TGA) – Australia
The Therapeutic Goods Administration (TGA) is a government regulatory authority overseeing the assessment, approval, and regulation of therapeutic goods including pharmaceuticals, medical devices, and biological products through the Therapeutic Goods Act 1989 of Australia. In order to lawfully supply the product in Australia, the good should be registered in the Australian Register of Therapeutic Goods (ARTG).
It is a significant pre-requisite that the foreign manufacturer should have appointed an Australian sponsor. An Australian Sponsor refers to a legally incorporated local entity that takes responsibility for the regulation of the product, management of ARTG registration, post market surveillance of the product and recall process.
Even though TGA carries out its own independent scientific assessment, the TGA has developed efficient abridged pathways.
The sponsors can use the abridged pathway via submitting evaluation reports from approved reference markets (like the FDA, EMA, Health Canada, and PMDA) to TGA, and this will considerably shorten the assessment time of the TGA.
The TGA also uses the Medical Device Single Audit Program (MDSAP).
9. Agência Nacional de Vigilância Sanitária (ANVISA) – Brazil
The Agência Nacional de Vigilância Sanitária (ANVISA), established by Law No. 9782 in December 1998, is an administratively independent, financially self-governing autarchy linked to the Ministry of Health. ANVISA possesses a exceptionally broad regulatory scope, supervising pharmaceuticals, active pharmaceutical ingredients (APIs), medical devices, food, cosmetics, pesticides, sanitizing agents, and tobacco products.
To market a health product in Brazil, foreign manufacturers must partner with a legally registered domestic company in Brazil to act as the marketing authorization holder. Under Brazilian law, marketing authorizations are valid for ten years.
To renew a registration, the MAH must submit a comprehensive data package, including post-market pharmacovigilance data, therapeutic ineffectiveness reports, domestic complaints, and long-term stability studies.
ANVISA enforces strict manufacturing quality standards, requiring physical, on-site GMP inspections of foreign active ingredient and finished dosage manufacturing sites unless specific mutual recognition or reliance protocols apply.
For commercial distribution, Brazil mandates serialization compliance, which includes the integration of ANVISA-specific verification holograms on product packaging to combat counterfeiting and ensure supply chain integrity.
10. Swissmedic – Switzerland
Swissmedic is the body operating under public law for the authorization and monitoring of human and veterinary medicinal products and medical devices in Switzerland according to the Therapeutic Products Act (TPA). Although the practices of Swissmedic used to be in line with the European Union regarding regulations, the lack of the renewal of the Mutual Recognition Agreement (MRA) between Switzerland and the EU has brought about significant consequences.
As a result of the fact that Switzerland does not have access to the European Database on Medical Devices (EUDAMED), Swissmedic has created independent measures of market control.
It involves the registration of the economic operator, the designation of Swiss Authorised Representative (CH-REP) for foreign medical device manufacturers and the use of the national registration database called Swissdamed that started registering medical devices from August 2025 with full compliance required by December 2026.
Swissmedic uses collaboration with other authorities, participating in the Access Consortium and Project Orbis for the maximization of the scope of reviews.
In terms of clinical trials, Swissmedic uses the FAST-Track procedure for conducting accelerated reviews of category B and C trials in coordination with competent Swiss ethics committees.
Comparative Matrix of Institutional Scope, Review Timelines, and Financial Architectures
To assist biopharmaceutical developers in planning multi-market submissions, the following tables provide a structured, comparative analysis of institutional landmarks, timeline metrics, statutory fees, and medical device classification systems.
Table 1: Institutional Profiles and Jurisdictional Mandates
| Authority | Headquarters | Primary Legislation | Regulatory Sub-Divisions & Technical Bodies | Scope of Jurisdictional Authority |
|---|---|---|---|---|
| US FDA[cite: 2] | Silver Spring, MD | FD&C Act; PDUFA VII | CDER (Drugs); CBER (Biologics); CDRH (Devices) | Drugs, Biologics, Devices, Food, Tobacco, Cosmetics |
| EMA[cite: 2] | Amsterdam, Netherlands | Regulation (EC) No 726/2004 | CHMP; Pharmacovigilance Risk Assessment Committee (PRAC) | Human & Veterinary Medicines (Centralized) |
| PMDA[cite: 2] | Tokyo, Japan | PMD Act (Revised 2025) | MHLW (Policy/Authorization); PMDA (Scientific Shinsa) | Drugs, Biologics, Devices, Regenerative Products |
| MHRA[cite: 2] | London, United Kingdom | Medicines Act 1968 | Clinical Trials Unit; Devices Division | Medicines, Medical Devices, Blood Components |
| CDSCO[cite: 2] | New Delhi, India | Drugs & Cosmetics Act 1940 | DCGI (Central CLA); State Licensing Authorities | Drugs, Biologics, Devices, Cosmetics, Clinical Trials |
| NMPA[cite: 2] | Beijing, China | Drug Administration Law | CDE (Drugs); CMDE (Devices); NIFDC (Testing) | Drugs, Biologics, Medical Devices, Cosmetics |
| Health Canada[cite: 2] | Ottawa, Canada | Food and Drugs Act | BRDD (Biologics); ROEB (Enforcement/HPCD) | Drugs, Biologics, Radiopharmaceuticals, Medical Devices |
| TGA[cite: 2] | Canberra, Australia | Therapeutic Goods Act 1989 | Medicines Regulation; Medical Devices & Quality | Medicines, Biologics, Devices, Scheduling of Chemicals |
| ANVISA[cite: 2] | Brasília, Brazil | Law No. 9782 (1998) | Medicines Office; Medical Devices Office | Medicines, APIs, Devices, Cosmetics, Tobacco, Food |
| Swissmedic[cite: 18] | Bern, Switzerland | Therapeutic Products Act | Licensing Division; Veterinary Medicines Department | Human & Veterinary Medicines, Medical Devices |
Table 2: Comparative Application Lifecycles and Timelines
The timelines indicated represent the active review clocks under standard and priority pathways, along with specialized clinical indicators and filing formats.
| Authority | Standard Review Timeline | Priority Review Timeline | Required Filing Format | Post-Market Commitment & Renewal Cycles |
|---|---|---|---|---|
| US FDA | 10 months | 6 months | eCTD | REMS implementation; Annual Reports |
| EMA | 210 active days | 150 active days | eCTD (Centralized) | PSUR filings; Periodic Safety Update reports |
| PMDA | 12 months | 9 months | eCTD (aligns with JP) | NHI re-pricing assessments |
| MHRA | 12 months | 150 working days | eCTD | Post-market registries; variation notifications |
| CDSCO | 12–18 months | 6–9 months | SUGAM / DDRS | Joint central/state post-market monitoring |
| NMPA | 12–18 months | 130 working days | Chinese Format / CDE eCTD | MAH annual reporting; adverse event tracking |
| Health Canada | 300 days | 180 days | eCTD | Shortage record keeping (1-year retention) |
| TGA | 255 working days | 150 working days | eCTD | Annual safety reports; PSUR submissions |
| ANVISA | 365 days | 120 days | ANVISA-specific dossier | 10-year renewal (stability & safety reports) |
| Swissmedic | 330–440 days | 140 working days | eCTD | Swissdamed operator/device registrations |
Table 3: Comparative Financial Schedules and Statutory Fees (FY 2025/2026)
The fees detailed reflect the high-range costs associated with initial New Active Substance (NAS) applications, clinical trials, or procedural consultations.
| Authority | New Active Substance Application Fee | Post-Marketing Variation / Maintenance Fee | Pre-Submission Consultation Fee | Financial Program / Inflation Adjustments |
|---|---|---|---|---|
| US FDA | $4,682,003 (FY 2026 rate with clinical data) | $442,213 (Prescription Drug Program Fee) | Free (Pre-IND / Pre-NDA alignments) | Base revenue $1.43B before inflation |
| EMA | €172,800 to €865,200 (Under Reg 2024/568) | Type II Variation: up to €163,200 | €51,900 to €98,400 (Scientific Advice) | SME deferrals; 30% Net Fee for re-examinations |
| PMDA | ¥46,901,700 (Review & Conformity) | ¥19,544,100 (Partial Changes) | ¥9,497,400 (Pre-application non-orphan) | Phase I consultation: ¥4,578,500 |
| MHRA | Dependent on the customized pathway | Low maintenance fee | Varies | Reduced fees for Access work-sharing |
| CDSCO | Subject to statutory sliding-scales | Sliding scale | Varies | Local manufacturing licensing scales |
| NMPA | Subject to CDE sliding-scales | Varies | Free (Breakthrough Therapies) | Mandatory laboratory testing fees |
| Health Canada | Subject to annual indexation | Varies | Free | Under HPCD review |
| TGA | Subject to annual indexation | ARTG annual charge | Varies | Abridged pathways reduce costs |
| ANVISA | Subject to RDC 753/2022 rates | RDC 73/2016 scales | Varies | Priority reviews do not incur surcharge |
| Swissmedic | Subject to TPA ordinances | Varies | FAST-Track clinical trial premium | Swissdamed registration fees apply |
Table 4: Comparative Medical Device Classifications and Regulatory Pathways
Regulatory frameworks classify medical devices into risk-based classes that dictate their technical dossier requirements and testing complexity.
| Device Type | US FDA Class | EU MDR Class | China NMPA Class | Brazil ANVISA Class | Australia TGA Class |
|---|---|---|---|---|---|
| Standard Scalpels | Class I (mostly exempt) | Class I (mostly) | Class I (Filing with SAMR) | Class I (Notification) | Class I (ARTG inclusion) |
| Powered Instruments | Class II (510(k)) | Class IIa | Class II (CDE Review) | Class II (Registration) | Class IIa |
| Hip/Knee Implants | Class III (PMA) / Class II | Class III | Class III (Central NMPA) | Class IV (High Risk) | Class III |
| Diagnostic Ultrasound | Class II | Class IIa | Class II | Class III | Class IIa |
| HIV Diagnostic Tests | Class II/III | Class D (IVDR) | Class III (Category 21/22) | Class IV (IVD) | Class III (IVD) |
| AI Diagnostic Software | Class II (SaMD) | Class IIa / IIb / III | Class II / III (SAMR catalog) | Class II / III | Class IIa / IIb / III |
Global Work-Sharing and Strategic Coalitions
To overcome resource challenges within the clinic, minimise duplication of effort, and facilitate faster pipeline review in the region, mature regulatory agencies have created highly integrated collaborative networks.
Project Orbis
Project Orbis was initiated by the FDA’s Oncology Center of Excellence (OCE) in May 2019 to facilitate the simultaneous submission and review of innovative cancer drugs with international regulatory partners. It is based on pre-existing bilateral confidentiality agreements.
The participants in this project are US FDA, Australian TGA, Health Canada, ANVISA (Brazil), HSA (Singapore), Swissmedic, MHRA of the UK, and the Ministry of Health in Israel.
There are three pathways for submissions depending on the timing relationship between the FDA and Project Orbis Partners (POPs):
- Type A (Fully Concurrent): Dossiers are submitted within 30 days of the FDA filing. This pathway enables multi-country review meetings, POP attendance at FDA clinical internal briefings, and high alignment on the final marketing authorization decision.
- Type B (Delayed Submission): Dossiers are submitted more than 30 days after the FDA filing. This allows POPs to conduct parallel assessments and share draft reviews, but the FDA final decision will occur first.
- Type C (Post-Approval Assessment): Submissions occur after the FDA has already approved the indication. The FDA continues to share its completed scientific assessments, but the POPs review the application independently, and POP teleconferences are not conducted.
While Project Orbis has significantly reduced submission lag times—demonstrated by a median timeline from FDA approval to UK MHRA approval of 172 days, and to Health Canada approval of 148 days—it does not mandate identical regulatory decisions. Regulators can reach divergent decisions, restrict or expand patient eligibility, or demand unique post-market commitments based on local standard-of-care comparators.
[PROJECT ORBIS ONCOLOGY PIPELINE]
|
____________________________|____________________________
| | |
v v v
[Type A] [Type B] [Type C]
Submit <= 30 Days Submit > 30 Days Post-FDA Approval
POP TCONs Conducted POP TCONs Conducted No Joint TCONs
Possible Concurrent Action FDA Decision First No Concurrent Action
The Access Consortium
Established in 2007 as the “ACSS” (Australia, Canada, Singapore, and Switzerland) and rebranded as “Access Consortium” in October 2020 due to the addition of the UK’s MHRA, the consortium can be described as a tightly coordinated cluster of medium-sized, highly mature regulators.
With the implementation of the NASWSI in 2018, sponsors need to provide an Expression of Interest (EOI) about the similarities of technical dossiers in all participating countries.
The regulators will be able to share responsibility in reviewing the common technical modules:
- One of the regulators will take charge of Module 3 (Quality/CMC).
- Another regulator will be responsible for Module 4 (Non-Clinical Toxicology).
- Yet another one will evaluate Module 5 (Clinical Safety and Efficacy).
Thus, the Access Consortium can prepare a single list of joint questions for the sponsor, reducing the work and time required for evaluation.
As part of its Strategic Plan 2025–2028, the Access Consortium offers its members access to a cloud-based workspace for joint reviews in real time.
The consortium also extended its portfolio of services by offering its scope through specialised networks for advanced therapy medicinal products (ATMPs) and biosimilars and a joint statement on GMP inspection reliance and recognition, which minimizes the need for duplicate facility audits.
The WHO Prequalification Programme (PQP)
The WHO Prequalification Programme (PQP), founded in 1987, is a unique procurement system which guarantees that the key health products correspond to internationally accepted criteria concerning their quality, safety, and efficacy.
Originally introduced for assessment of the childhood vaccines acquired by UNICEF, the PQP later became involved in evaluation of the active pharmaceutical ingredients (APIs), generic medicines (with emphasis on the most burdensome diseases such as HIV, malaria, and tuberculosis), in vitro diagnostics, refrigerators for immunization purposes, and vector control products.
Notably, the PQP does not constitute a sovereign licensing organisation; therefore, it operates on the basis of strict conditions.
For instance, the vaccine prequalification process admits applications from the manufacturers whose National Regulatory Authority (NRA) was found qualified and functioning well (GBT Maturity Level 3 or 4).
Such an approach has become a strong motivator for developing countries to create their own regulatory systems in order to guarantee a safe manufacturing base in these countries.
Future Horizons: The Bio-Digital Frontier and Bayesian Paradigms
The integration of advanced technologies, such as artificial intelligence (AI), multi-omics datasets, digital twins, and real-world evidence (RWE), is transforming the baseline requirements for regulatory validation. Regulators are adapting their assessment methodologies to accommodate these highly sophisticated, data-driven approaches.
Bayesian Inference and Justification-First Clinical Designs
In January 2026, the FDA of the US issued a draft guidance on Bayesian statistics in the context of drug and biological product clinical trials. This is a marked departure from the existing frequentist trial paradigm (where only the use of p-values and large numbers of patients in the cohort are involved) towards a paradigm where prior scientific knowledge can be systematically utilized.
Posterior Probability P(θ|D) ∝ Likelihood P(D|θ) x Prior Probability P(θ)
Within the Bayesian paradigm, clinical studies from the past, preclinical multi-omics datasets, and real-world data are mathematically combined to obtain the “prior probability”.
The “prior probability” is then combined with the likelihood obtained through a new, very focused clinical study to obtain the “posterior probability”.
This rationale-first approach becomes highly relevant in cases where conducting a large scale clinical trial is either difficult or unethical:
- Orphan and Rare Diseases: Whereby sponsors can use the data from limited pediatric trials in combination with prior adult efficacy.
- Biosimilars: Whereby sponsors can integrate the information from analytical chemistry, PK profiles, and real-world clinical experience.
Real-Time Clinical Trials (RTCT) and Adaptive Oversight
In order to mitigate the lengthy period from completion of trial until final regulation, the FDA is exploring an approach to Real-Time Clinical Trials (RTCT) through partnerships with oncology sponsors. The concept involves dynamic data pipeline that sends safety and efficacy signals in near-real-time directly to the regulator, unlike traditional static dossiers.
Regulators are also creating validation frameworks for AI and machine learning (ML) models. Validation will be needed for “digital twins” of human physiology to predict disease progression and simulate treatment response as well as for AI synthetic control arms that eliminate physical control arms.
Feasibility of RTCT and validation of AI models require sponsor demonstration of readiness on three dimensions:
- Operational Readiness: Sponsors have to develop secure data pipeline infrastructure that will convert site data into structured, regulation visible signal notifications, without revealing trial blinding and protecting patient privacy.
- Governance Readiness: More transparency requires better control frameworks for validation and auditing of the algorithm for potential issues such as data drift, clinical bias and model integrity.
- Evidence Readiness: Sponsors have to provide scientific rationale for using AI in design or monitoring as improvement in clinical decision-making quality, not only time efficiency.
Strategic Conclusions for Global Biopharmaceutical Sponsors
Success in today’s regulatory landscape necessitates a highly evolved regulatory intelligence strategy that recognizes the registration process worldwide as an intricate, interconnected, multi-market puzzle and not a set of individual market registrations.
Early Collaboration on Harmonization Efforts
Sponsors need to engage with initiatives such as Access Consortium and Project Orbis from the early stages of design of their clinical trials, since designing a protocol that will satisfy both the clinical requirements of FDA, the local data requirement of PMDA, as well as the specifications of Chinese and Brazilian pharmacopeia, is key to preventing delays.
Early-stage consultation
The early consultation phase through regulatory sciences consultations with PMDA, Pre-IND alignments with FDA, and PRIME initiative with EMA is the best way to predict the time of approval of a product. Early alignment of clinical strategy as well as CMC strategy with the regulator’s expectations before locking the protocols will prevent CRLs.
Adoption of Real-World Evidence and Bio-Digital Approaches
As regulators develop guidance regarding Bayesian design, RWE and AI-enabled clinical trials, biopharmaceutical companies must develop the capability to collect and analyze data.